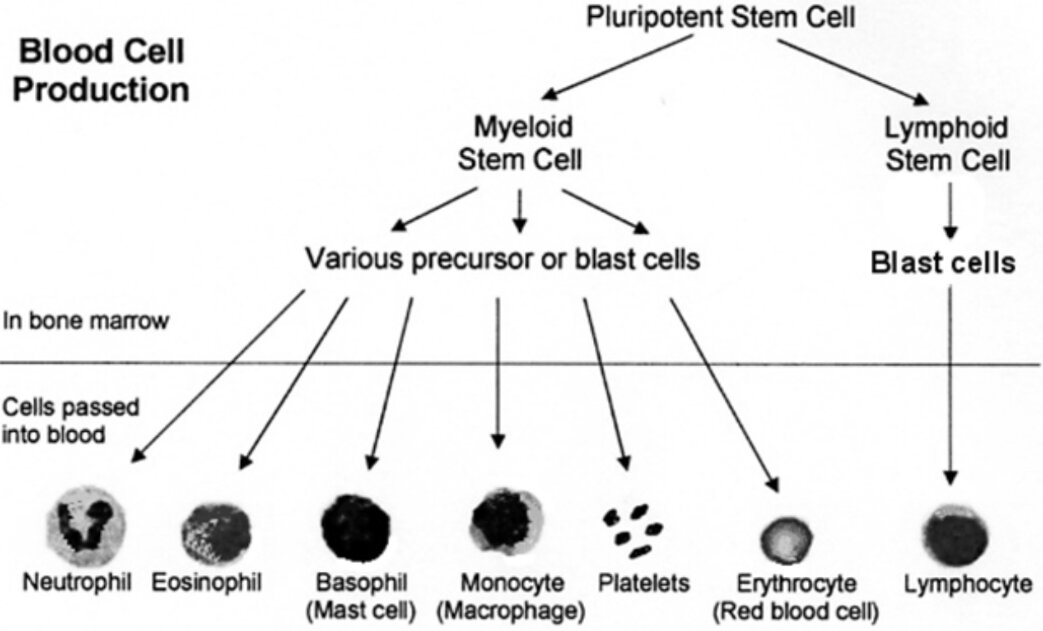
Overview haematological malignancies (leukaemia, lymphoma and myeloma)
Introduction
33% of all haematological malignancies are diagnosed via the emergency route, which is much higher than the average of 23 for all other cancers.
One year survival for cancers that presented via emergency route was lower than those diagnosed via 2ww: 51% vs 82% (Myeloma); 50% vs 85% (NHL).
ALL is the most common cancer in children 0-14y and lymphoma is the most common cancer in teenagers/young adults 15-24y
New cases diagnosed per year in the UK
GP is likely to diagnose around 1-2 cases of haematological cancer every 2 years.
Overall, around 32,000 new cases of haematological malignancy
Non-Hodgkin’s lymphoma 13,000
Leukaemia 8,000
Myeloma 4,500
Hodgkin’s lymphoma 2,000
“NICE has lowered the threshold for cancer investigations and referral to achieve ≥3% PPV”
Prevalence
NHL Non-Hodgkin’s lymphoma 43%
MM Multiple Myeloma 17%
CLL Chronic Lymphocytic Leukaemia 13%
AML Acute Myeloid Leukaemia 10%
HL Hodgkin’s Lymphoma 6%
ALL Acute Lymphoblastic Leukaemia 2%
Others 9%
Presenting symptoms
Any combination of
Fatigue
B (systemic) symptoms: fever, night sweats, shortness of breath, pruritus, weight loss or alcohol-induced lymph node pain (specific to Hodgkin Lymphoma)
Lymphadenopathy (localised or generalised) or hepatomegaly or splenomegaly
Other symptoms:
Skin pallor, bruising, petechiae
GIT abdominal pain
MSK bone Pain
Unexplained bleeding
Recurrent infections
Q-Cancer risk assessment tool
Assessment
Examination
Full physical examination, examine for lymphadenopathy (cervical, axillary, inguinal) and hepatosplenomegaly
Investigations
Urgent
FBC Full blood count
U&Es, LFTs, clotting screen
Lactate Dehydrogenase LDH, elevated uric acid
CRP and ESR
CXR for lymphadenopathy or mediastinal mass
HIV, Hepatitis B and C serology
Myeloma screen
Calcium
Plasma viscosity or ESR
Serum protein electrophoresis and Bence-Jones protein urine test
Non-Hodgkin’s lymphoma (commonest haematological malignancy)
Generalised lymphadenopathy, splenomegaly AND B (systemic) symptoms
Pathology: malignancy of B-lymphocytes (85-90% cases) or T-lymphocytes
Risk factors: HIV, Human Herpes virus 8, H.Pylori, Hepatitis C, EBV (Burkitt’s)
Age: 50-70y
5-year survival 70%, responds to Rituximab (monoclonal antibody to B cell)
Hodgkin’s lymphoma
Localised lymphadenopathy (painless cervical), splenomegaly, mediastinal mass (CXR) AND B (systemic) symptoms
Pathology: malignancy of B-lymphocytes
Risk factors: immunocompromised, previous EBV infection
Age: 1st peak 15-24y & female, 2nd peak >50y & male
5-year survival 85%
Leukaemia:
Common signs of leukaemia include anaemia, reduced normal white cells and thrombocytopaenia.
The most common symptoms of leukaemia include pallor, bruising, bleeding, petechiae, hepatosplenomegaly and a propensity to infection.
Many chronic leukaemias are symptomless and are only identified when a full blood count is performed for other reasons.
5-year survival 52%
ALL
Presentation: fatigue, bone pain, recurrent infections, LUQ fullness (splenomegaly), shortness of breath, headache, bleeding (nose bleeds, menorrhagia, bruising)
Risk factors: genetic, trisomy 21, radiation exposure
Prognosis: intensive chemotherapy achieves long-term survival rate of 85%
AML
Presentation: fever, bleeding, splenomegaly, leukostasis (WBC>100 causing respiratory distress and altered mental status), bone pain, petechiae, gingivitis
Investigations: High WBC count, neutrophils very low, anaemia, thrombocytopenia; high LDH
Risk factors: myelodysplastic syndromes, polycythaemia rubra vera, paroxysmal nocturnal haemoglobinuria, aplastic anaemia
Prognosis: intensive chemotherapy achieves long-term remission rates of 60-70%
CLL
Presentation: lymphadenopathy or hepatosplenomegaly, Non-specific B symptoms, pruritus, recurrent infections; around 25-50% are asymptomatic at presentation
Investigations: chronically elevated lymphocytes; monoclonal B-lymphocytes
Risk factors: Age>60y
Prognosis: relatively indolent cancer, patients live >20yr; treatment with Rituximab (monoclonal antibody to B cell);
All CLL patients should receive vaccinations: HiB, meningococcal C, pneumococcus, influenza (Shingles vaccine is contraindicated as it is a live vaccine)
CML
Presentation: lethargy, splenomegaly, Non-specific B symptoms, pruritus
Investigations: chronically elevated leucocytes (neutrophils, basophils, eosinophils); elevated uric acid and ALP
Risk factors: Age>60y
Prognosis: treatment with tyrosine kinase inhibitors such as Imatinib
Myeloma
Symptoms include
fever, anaemia, weight loss, hepatomegaly
recurrent/persistent infections with encapsulated organisms (streptococcus pneumoniae, haemophilus influenzae)
bone pain, often in multiple sites such as the ribs, and bone marrow failure
pathological fracture (26-34% of patients) following minimal trauma, especially of the femoral neck
lower limb weakness and paraesthesia due to vertebral compression
symptoms of hypercalcaemia (nausea, fatigue, confusion, abdominal pain, polyuria, renal calculi)Perform myeloma screen if >60yr + persistent bone pain (particularly back pain) or unexplained fracture or hypercalcaemia or leucopenia
Consider myeloma screen >60y with renal dysfunction and anaemia
Complications are consequent to paraproteinaemia: kidney failure, peripheral neuropathy, hyper-viscosity leading to thromboembolism.
Treatment includes specific disease directed therapy (e.g. Bortezomib, thalidomide, lenalidomide) and supportive therapy (e.g. transfusion, antibiotics, plasmaphoresis for hyper viscosity, radiotherapy for localised painful lesions)
5-year survival 50%
Side-effects of cancer therapies
Bisphosphonates: facial swelling, leg swelling, muscle cramps, rash, flu-like symptoms
Steroids: weight gain, infection, mood changes, thinning of skin, muscle weakness, Cushing’s syndrome, osteoporosis, diabetes, hypertension
Radiotherapy: localised soreness, anorexia
Chemotherapy: fatigue, hair loss, anaemia, mucositis from mouth to anus, infertility, myelosuppression
Novel therapies: neuropathies, colitis, periorbital and peripheral oedema, myelosuppression
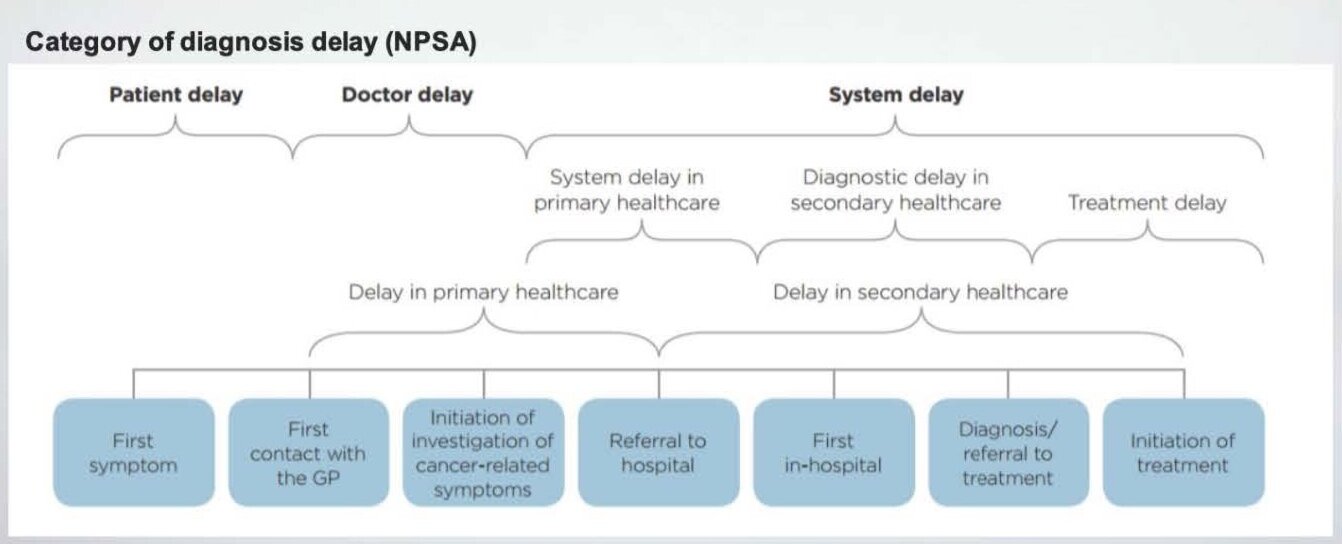
Routes to diagnosis
Improved survival requires diagnosis at an early stage, early access to optimal treatment and improvements in the management of co-morbidity of older people.
Factors contributing to international differences in cancer survival include
More advanced stage at diagnosis
Delays in diagnosis and treatment
Treatment variation
Co-morbidity
Reasons for delayed diagnosis
Patient interval: age, sex, socio-economic status and patients’ beliefs about cancer and cancer symptoms, non-specific nature of symptoms
Doctor interval: failure to link previous repeated/multiple presentations, lack of continuity of care, confounding effects of co-morbid disease, failure to follow referral guidelines.
Number of pre-referral GP consultations
27.6% of people with haematological cancer saw their GP three or more times before referral.
However, only 3.9% of patients with breast cancer saw their GP three or more times before referral.